
Vitamin D Benefits: Most people who think about vitamin D think about bones. Maybe sunlight. Maybe a supplement their doctor mentioned once. And technically, none of that is wrong — but it misses the bigger picture almost entirely.
Here’s what the research increasingly shows: the real problem with vitamin D isn’t the dramatic deficiency that causes rickets or osteomalacia. It’s the quiet, widespread insufficiency sitting in the gray zone — blood levels that look “acceptable” on a standard lab report but are nowhere near what the body actually needs to regulate immunity, mood, hormonal balance, sleep, and long-term disease risk. Roughly 35% of adults carry levels below the threshold most clinicians flag as deficient, and a far larger portion never reaches what researchers associate with genuine functional benefit. They feel tired. They get sick more often than they should. Their mood dips in ways that are hard to explain. And they rarely connect any of it to vitamin D.

This post covers the full picture of vitamin D benefits as the current science understands them — from bone health and immune modulation to testosterone, depression, sleep, and cardiovascular function. It also covers what most content on this topic gets wrong: the difference between avoiding deficiency and actually optimizing your levels, the forms that matter, the dosing questions that don’t have simple answers, and why getting more sun is often less effective than people assume.
What Is Vitamin D, Really?
The name is misleading. Vitamin D is classified as a vitamin, but it behaves almost nothing like one. True vitamins are compounds the body cannot synthesize on its own — they must come from food. Vitamin D, by contrast, is produced in human skin when exposed to ultraviolet B radiation from sunlight. Once activated, it functions as a steroid hormone, binding to receptors in virtually every tissue in the body and influencing the expression of hundreds of genes. Calling it a vitamin undersells what it actually does.
The Difference Between Vitamin D and a True Vitamin
When vitamin D enters the bloodstream — whether synthesized through sun exposure or absorbed from a supplement — it travels to the liver, where it is converted into 25-hydroxyvitamin D, the storage form measured in blood tests. From there, the kidneys convert it into calcitriol (1,25-dihydroxyvitamin D), the biologically active hormone that does the real work.
Calcitriol binds to the vitamin D receptor (VDR), a nuclear receptor found in tissues across the entire body — bone, muscle, immune cells, brain, heart, colon, prostate, and more. Once bound, it acts directly on gene expression. This is not a peripheral nutrient with a narrow job description. It is a regulatory molecule with system-wide reach, and that is precisely why deficiency produces such a broad and diffuse set of symptoms.
Vitamin D2 vs. D3: Which Form Actually Works
Two forms are commonly found in supplements: vitamin D2 (ergocalciferol), derived from plant sources and fungi, and vitamin D3 (cholecalciferol), the form synthesized in human skin and found in animal-based foods. They are not equivalent in practice.
Multiple comparative studies have demonstrated that vitamin D3 raises serum 25-hydroxyvitamin D levels more effectively and sustains them for longer than D2. A 2012 meta-analysis published in the American Journal of Clinical Nutrition confirmed this superiority, showing D3 was approximately 87% more potent at raising and maintaining circulating vitamin D levels. The lower affinity of D2 metabolites for vitamin D-binding protein likely accounts for faster clearance from the bloodstream.
For supplementation purposes, vitamin D3 is the standard recommendation among most nutrition researchers and clinicians. It is the form used in the majority of high-quality clinical trials and the one you will find in nearly every well-formulated supplement today.
How Your Body Makes and Activates Vitamin D
When UVB radiation from sunlight hits the skin, it converts a cholesterol precursor — 7-dehydrocholesterol — into pre-vitamin D3, which is then thermally isomerized into vitamin D3. This process is highly variable. Skin pigmentation, geographic latitude, season, time of day, age, sunscreen use, and body composition all affect how much vitamin D is actually synthesized from a given amount of sun exposure.
Once vitamin D3 reaches the liver and is converted to 25-hydroxyvitamin D, the kidneys complete the activation to calcitriol under the influence of parathyroid hormone (PTH) and blood calcium and phosphate levels. This tight regulatory feedback loop is one reason that measuring 25-hydroxyvitamin D in a blood test gives a reliable picture of overall vitamin D status — it reflects both dietary intake and sun-derived synthesis over the preceding weeks.
How to Get Vitamin D from Food — and Why It’s Rarely Enough
Before the supplement conversation begins, there is a reasonable question worth answering directly: can you simply get enough vitamin D from food?
The short answer is: for most people, no. Not reliably, and not without a diet that is very specifically structured around a narrow set of foods that most people do not eat in sufficient quantities every day. Understanding why starts with looking at what the food sources actually provide.
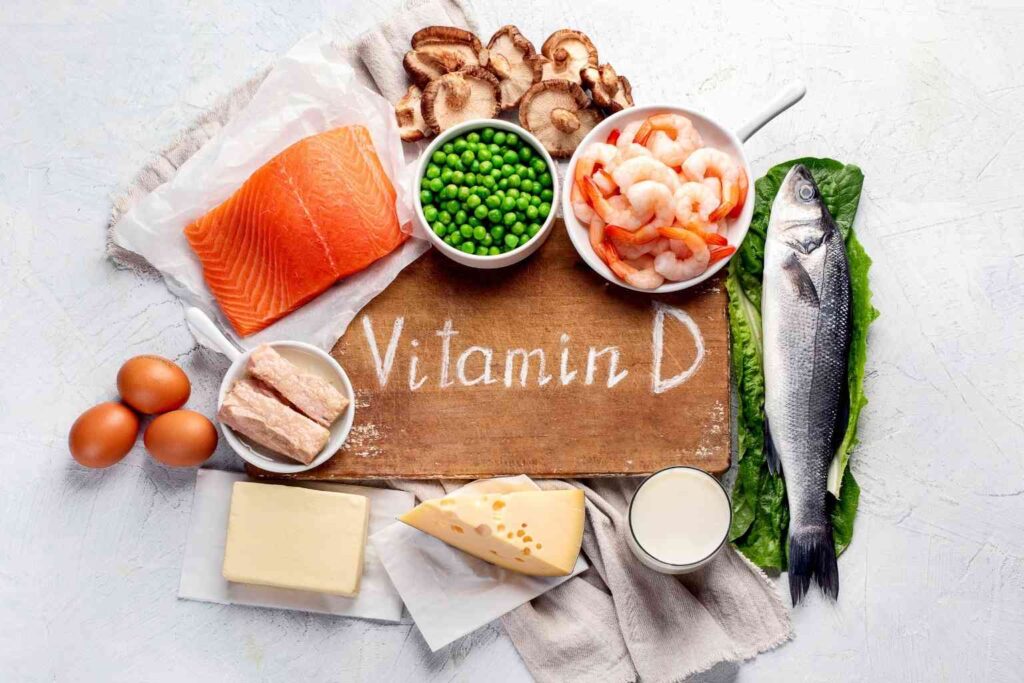
The Best Dietary Sources of Vitamin D
Vitamin D is one of the least abundant nutrients in the general food supply. Unlike vitamins C or B12, which appear across a wide variety of plant and animal foods, vitamin D is concentrated in a small number of specific sources — almost all of them animal-based.
Fatty fish are by far the richest natural source. A 3.5 oz (100g) serving of wild-caught salmon provides approximately 600–1,000 IU of vitamin D3, depending on whether it is wild or farmed — wild salmon consistently delivers more. Swordfish offers around 700 IU per serving. Canned tuna provides a more modest 150–230 IU. Sardines and mackerel fall in the 300–500 IU range per serving.
Cod liver oil is the single most concentrated food-based source, delivering approximately 400–1,000 IU per teaspoon depending on the product. It has been used historically as a vitamin D and omega-3 source, though its strong flavor limits daily use for many people.
Egg yolks contribute roughly 40–50 IU per yolk — meaningful as part of a varied diet, but far from sufficient as a standalone source. Eggs from pasture-raised hens exposed to sunlight tend to provide more than conventional eggs, with some research showing two to four times higher levels.
Beef liver offers approximately 40–50 IU per 3.5 oz serving — similar to eggs, and with the same limitation of providing only a minor contribution to daily needs.
Fortified foods are where most people in Western diets incidentally encounter vitamin D. Fortified cow’s milk typically provides 100–130 IU per cup. Fortified plant milks vary significantly by brand but are generally in a similar range. Fortified cereals and orange juice contribute 40–100 IU per serving. These amounts are better than nothing — but they were designed to prevent severe deficiency, not to optimize levels.
UV-exposed mushrooms are the only meaningful plant-based source. When mushrooms are exposed to ultraviolet light — either commercially or by placing them gill-side up in direct sunlight for 15–30 minutes — they synthesize vitamin D2 in amounts that can reach 400 IU or more per 3.5 oz serving. This conversion is genuine and measurable, though D2 is less potent than D3 at raising serum levels.
When Diet Alone Falls Short
Here is the practical problem. The current research suggests that maintaining serum 25-hydroxyvitamin D levels in the functional optimum range — roughly 30–50 ng/mL — typically requires a daily intake in the range of 1,000–2,000 IU or more, depending on baseline levels, body weight, and sun exposure.
Reaching even 1,000 IU from food alone on a consistent daily basis requires eating fatty fish multiple times per week, every week, year-round. Most people do not. The average dietary vitamin D intake in adults eating a typical Western diet is estimated at 150–300 IU per day — a fraction of what most researchers now consider adequate for non-skeletal benefits.
For specific dietary patterns, the gap is even wider.
Vitamin D and Dietary Restrictions
Vegans and strict vegetarians face the most significant structural barrier. Fatty fish, the richest natural sources, are entirely excluded. Eggs and dairy contribute modest amounts but are also excluded in vegan diets. UV-exposed mushrooms and fortified plant milks are available options, but rarely sufficient on their own. A well-designed 2021 study published in Nutrients found that vegans had significantly lower serum 25-hydroxyvitamin D levels than omnivores, with a substantially higher prevalence of deficiency — a gap that persisted even after accounting for sun exposure differences.
People with fish or seafood allergies lose access to the most concentrated food-based sources by default, leaving fortified foods and eggs as the primary dietary options — neither of which comes close to covering daily needs independently.
People who avoid dairy — whether due to lactose intolerance, milk protein allergy, or dietary preference — lose the fortified milk contribution that provides a meaningful baseline for many Western diets. Plant-based milks vary widely in their fortification levels, and not all are fortified at all.
Older adults face a compounding challenge: not only does sun synthesis decline sharply with age, but dietary variety often narrows, and the gut’s efficiency at absorbing fat-soluble nutrients decreases. The people who most need to maintain adequate vitamin D levels are often the least equipped to do so through food and sun alone.
The conclusion is not that food sources are irrelevant — they contribute, and a diet rich in fatty fish, eggs, and fortified foods is meaningfully better than one without them. The conclusion is that for most adults outside of very specific dietary patterns and geographic contexts, food alone is an unreliable strategy for reaching and maintaining the vitamin D levels that the research associates with genuine functional benefit. Supplementation in this context is not a replacement for a good diet. It is the practical correction for a gap that diet and sunlight, for most people, simply cannot reliably close.
Vitamin D Deficiency Symptoms Most People Miss
The challenge with vitamin D deficiency is that most of its symptoms are nonspecific. Fatigue, low mood, muscle weakness, frequent infections — these are complaints that fit dozens of conditions. They rarely prompt a doctor to immediately order a vitamin D test, and they rarely prompt patients to connect the dots themselves.

The Classic Symptoms — and Why They Show Up Late
The textbook symptoms of severe vitamin D deficiency are well-documented: bone pain, muscle weakness, increased fracture risk, and in children, rickets. In adults, prolonged severe deficiency leads to osteomalacia — a softening of the bones caused by inadequate mineralization. These are real and serious outcomes, but they represent the endpoint of prolonged, significant deficiency. Most people are not there.
What is far more common is the cluster of symptoms associated with moderate or subclinical deficiency: persistent fatigue that does not resolve with adequate sleep, diffuse musculoskeletal aching, frequent upper respiratory infections, low mood or seasonal mood changes, and impaired concentration. A 2022 review published in Nutrients noted that even modest reductions in serum 25-hydroxyvitamin D are associated with measurable increases in inflammatory markers and impairments in immune cell function — effects that precede any structural bone damage by years.
Subclinical Deficiency: The Gap Nobody Talks About
Here is where the real problem lies for most adults. The conventional deficiency threshold — a serum 25-hydroxyvitamin D level below 20 ng/mL — was established primarily in relation to bone health. Getting above that number protects the skeleton. But a growing body of research suggests that the threshold for optimal function in immune regulation, mood, hormonal balance, and cardiovascular health may be meaningfully higher — somewhere between 30 and 50 ng/mL, depending on the health outcome in question.
A 2025 review published in Nutrients analyzed dose-response data across dozens of meta-analyses and found that risk reduction for outcomes including cancer mortality, cardiovascular disease, respiratory infections, and depression continued to improve with serum levels well above the conventional deficiency cutoff. Many people sitting at 22 or 25 ng/mL — technically “sufficient” by standard lab reference ranges — may be operating at a significant disadvantage for non-skeletal health outcomes.
That gap is where the optimization question actually lives. And it is the conversation that most content on vitamin D benefits never quite gets to.
Vitamin D Deficiency and Hair Loss: What the Research Says
One of the less commonly discussed associations involves hair follicle cycling. Vitamin D receptors are expressed in hair follicle keratinocytes, and animal studies have consistently shown that VDR knockout models develop alopecia. In humans, observational data links low serum 25-hydroxyvitamin D with alopecia areata — an autoimmune form of hair loss — as well as with diffuse telogen effluvium.
A 2019 review in Dermatology and Therapy found that patients with alopecia areata had significantly lower vitamin D levels than controls, and that supplementation in deficient patients was associated with reduced disease severity. The evidence is observational and not yet sufficient to claim vitamin D supplementation as a hair loss treatment, but the biological rationale is solid enough to make it a relevant consideration for anyone experiencing unexplained hair thinning alongside other possible deficiency markers.
Vitamin D Benefits: What the Research Actually Shows
The evidence base for vitamin D benefits is large, complex, and sometimes contradictory. Observational studies consistently show associations between higher serum levels and better outcomes across nearly every disease category. Randomized controlled trials produce more mixed results — partly because many were designed around populations that were not actually deficient, limiting the effect size available to measure. Understanding that nuance is essential for reading the literature honestly.
1. Bone Health and Calcium Absorption
This is the most established vitamin D benefit and the one with the longest research history. Vitamin D is essential for intestinal calcium absorption — without adequate levels, the gut absorbs as little as 10–15% of dietary calcium, compared to 30–40% when vitamin D status is sufficient. The difference is not trivial. Chronic low absorption drives compensatory increases in parathyroid hormone, which draws calcium from bone to maintain serum levels, accelerating bone loss over time.

A 2022 Cochrane review of vitamin D supplementation for fracture prevention found modest but meaningful reductions in hip fracture risk, particularly in older adults and those with baseline deficiency. Vitamin D alone without calcium showed weaker effects; the combination performed consistently better. For anyone concerned about bone density — especially postmenopausal women and men over 60 — maintaining adequate vitamin D status is not optional. It is foundational.
2. Immune System Modulation
The vitamin D and immune system connection has attracted significant research attention, particularly since the COVID-19 pandemic brought widespread interest in immune-modulating nutrients. The biology is well-established: vitamin D receptors are expressed on virtually every immune cell, including T cells, B cells, and macrophages. Calcitriol directly regulates the expression of antimicrobial peptides like cathelicidin, which play a front-line role in innate immune defense.
A 2017 meta-analysis of 25 randomized controlled trials published in The BMJ — involving over 11,000 participants — found that vitamin D supplementation reduced the risk of acute respiratory tract infections by 12% overall, with a stronger 70% reduction in individuals who were severely deficient at baseline. Daily or weekly supplementation showed protective effects; large bolus doses did not. The dosing pattern matters here, not just the total amount.
3. Mood, Mental Health, and Depression
The relationship between vitamin D and depression is among the most researched of its non-skeletal benefits. Vitamin D receptors are found throughout the brain, including in regions associated with mood regulation. Calcitriol influences the synthesis of serotonin — a neurotransmitter central to emotional regulation — by upregulating the gene that encodes tryptophan hydroxylase 2, the enzyme that produces it in the brain.

Observational data is consistent: low serum vitamin D correlates with higher rates of depressive symptoms across populations. Intervention data is more nuanced. A 2023 meta-analysis in Critical Reviews in Food Science and Nutrition found that vitamin D supplementation produced significant improvements in depression scores in individuals with clinically diagnosed depression, but showed weaker effects in general population studies without pre-existing diagnosis. The takeaway is not that vitamin D is an antidepressant — it is that correcting genuine deficiency in depressed individuals appears to matter clinically, while supplementing people with already-adequate levels produces smaller effects.
4. Testosterone and Male Hormonal Health
This is a vitamin D benefit that rarely gets adequate attention in mainstream wellness content. Vitamin D receptors are present in Leydig cells — the testicular cells responsible for testosterone synthesis — and research has found a meaningful correlation between serum 25-hydroxyvitamin D and circulating testosterone levels in men.
A 2011 RCT published in Hormone and Metabolic Research found that men supplementing with 3,332 IU of vitamin D daily for one year experienced significantly higher testosterone levels compared to placebo — an increase of approximately 25% from baseline. A 2020 systematic review and meta-analysis in Journal of Steroid Biochemistry and Molecular Biology confirmed the association between vitamin D status and testosterone, noting that deficient men showed the most robust response to supplementation.
For men over 50 experiencing the gradual decline in testosterone that accompanies aging — and the fatigue, reduced libido, and mood changes that often follow — ensuring adequate vitamin D status is a low-cost, evidence-supported first step before considering more aggressive hormonal interventions.
5. Sleep Quality and Circadian Regulation
The connection between vitamin D and sleep is less widely known but biologically plausible. Vitamin D receptors are present in brain regions involved in sleep regulation, including the hypothalamus and areas associated with circadian rhythm control. Vitamin D also influences the production of melatonin indirectly through its effects on the sleep-wake cycle regulatory pathways.

A 2018 randomized controlled trial published in Sleep Medicine found that vitamin D supplementation in deficient participants significantly improved sleep quality, reduced sleep latency, and increased total sleep duration compared to placebo. A 2023 cross-sectional analysis using NHANES data found that adults with serum 25-hydroxyvitamin D below 20 ng/mL reported significantly worse sleep quality and shorter sleep duration than those with sufficient levels.
The practical implication here is underappreciated: persistent sleep difficulties in adults are often investigated through the lens of stress, screen time, or sleep hygiene — rarely through nutritional status. Vitamin D deficiency is a legitimate contributor to sleep disruption that is worth ruling out before assuming behavioral causes.
6. Cardiovascular Health
Cardiovascular disease is the leading cause of death in most high-income countries, and vitamin D has emerged as a relevant factor in cardiac risk. Vitamin D receptors are expressed in cardiomyocytes and vascular smooth muscle cells. Calcitriol plays a role in regulating renin — the enzyme at the top of the renin-angiotensin-aldosterone system that governs blood pressure — and influences inflammatory pathways implicated in atherosclerosis.
Large observational studies consistently show that low serum 25-hydroxyvitamin D is associated with higher risk of hypertension, heart failure, and cardiovascular mortality. RCT data is mixed, with the large VITAL trial finding no significant reduction in major cardiovascular events from vitamin D supplementation in a generally healthy population. However, subgroup analyses and more recent 2025 meta-analyses — including a narrative review published in Nutrients examining data from studies controlling for baseline deficiency — suggest that benefits are more apparent in individuals who begin supplementation with genuinely low levels. The pattern mirrors what is seen in immune and mood research: correction of deficiency matters; supplementing already-replete individuals produces weaker effects.
7. Inflammation and Chronic Disease Risk
Chronic low-grade inflammation is the underlying driver of most major non-communicable diseases — cardiovascular disease, type 2 diabetes, certain cancers, and neurodegenerative conditions. Vitamin D exerts meaningful anti-inflammatory effects through multiple pathways: suppressing pro-inflammatory cytokines including TNF-alpha and IL-6, reducing NF-kB signaling, and promoting regulatory T cell activity that keeps immune responses from becoming self-destructive.

A landmark observational analysis published in Nutrients in January 2025 — examining NHANES data covering 47,478 individuals — found that higher 25-hydroxyvitamin D levels were associated with lower mortality from eight of the ten leading causes of death in the studied population, including cancer, stroke, chronic lower respiratory disease, Alzheimer’s disease, and kidney disease. Associations remained after adjustment for age, BMI, diabetes, and hypertension. This is observational data, not proof of causation — but the consistency and breadth of the signal across disease categories is difficult to dismiss.
8. Weight Management and Metabolic Health
The relationship between vitamin D and body weight runs in both directions. Obesity is one of the strongest independent risk factors for vitamin D deficiency — adipose tissue sequesters vitamin D, reducing its bioavailability regardless of intake or sun exposure. At the same time, low vitamin D status appears to impair metabolic function in ways that may contribute to weight gain.

Vitamin D receptors are present in adipocytes, and calcitriol influences fat cell differentiation and storage. Low vitamin D has been associated with higher levels of parathyroid hormone, which promotes fat storage and inhibits lipolysis. Some research also suggests a connection between vitamin D status and insulin sensitivity — though RCT evidence for weight loss from supplementation alone remains inconsistent. A 2020 meta-analysis in Obesity Reviews found no significant independent effect of vitamin D supplementation on weight loss in general populations, but noted that deficient individuals correcting their levels showed metabolic improvements that may support weight management as part of a broader lifestyle approach.
Vitamin D and the Sunshine Paradox: Why More Sun Doesn’t Always Solve the Problem
Sunlight is the most natural source of vitamin D, and the conventional advice — get more sun — sounds simple enough. The reality is considerably more complicated.
For UVB radiation to trigger vitamin D synthesis in the skin, the sun needs to be at a sufficient angle above the horizon. In practice, this means that at latitudes above roughly 35 degrees north or south, meaningful vitamin D synthesis is limited or impossible during winter months — regardless of how much time someone spends outside. A person living in northern Europe, Canada, or the northern United States can be outdoors for hours on a December afternoon and produce essentially no vitamin D from that exposure. The UVB component simply is not present at that sun angle.
Even in sunnier climates and favorable seasons, several factors dramatically reduce vitamin D synthesis. Skin pigmentation is one of the most significant — melanin acts as a natural sunscreen, and people with darker skin tones require substantially more sun exposure to produce equivalent amounts of vitamin D compared to those with lighter skin. Research suggests that individuals with very dark skin may need five to ten times more sun exposure to achieve the same synthesis rate.
Age compounds the problem. The skin’s capacity to synthesize vitamin D from UVB exposure declines progressively with age — by approximately 75% between the ages of 20 and 70. An older adult spending the same amount of time in the sun as a younger person produces a fraction of the vitamin D. This partially explains why vitamin D insufficiency is so prevalent in adults over 60 even in regions with adequate sunshine.
Sunscreen, which is increasingly recommended for skin cancer prevention, further reduces synthesis. SPF 15 reduces vitamin D production by approximately 99%. The advice to protect skin from UV damage and the advice to get more vitamin D from sunlight are in direct tension — a tension that is rarely acknowledged clearly in either dermatological or nutritional guidance.
There is also the realistic question of compliance. Meaningful vitamin D synthesis from sun exposure requires large areas of skin — arms, legs, torso — to be uncovered during peak UVB hours. For many people — those who work indoors, those in colder climates, those who cover skin for cultural or religious reasons — relying on sun exposure as a primary vitamin D source is simply not practical for a significant portion of the year.
This is the sunshine paradox: the natural solution works, but only under a set of conditions that a large portion of the global population does not reliably meet. Supplementation fills the gap not as a shortcut but as a practical correction for real-world limitations.
Who Benefits Most from Vitamin D Supplementation
Vitamin D supplementation is not equally valuable for everyone. The people who stand to benefit most are those whose baseline levels are lowest — which correlates predictably with specific life circumstances, demographics, and health profiles.
Adults Over 50 — Women
Postmenopausal women face a convergence of risk factors that make vitamin D optimization particularly relevant. Estrogen decline accelerates bone turnover, and calcium metabolism becomes less efficient. Vitamin D’s role in maintaining intestinal calcium absorption becomes more critical precisely when the hormonal support for bone maintenance is declining. Low vitamin D in this population directly compounds fracture and osteoporosis risk.
Beyond skeletal health, observational data consistently links lower vitamin D levels in postmenopausal women with higher rates of depression, cognitive decline, and cardiovascular events. Vitamin D deficiency symptoms in women over 50 are often attributed to menopause itself — fatigue, mood changes, joint discomfort — when a straightforward blood test might reveal a correctable nutritional gap underneath.
Men Over 50 — Hormones, Prostate, and Vitality
For men, the testosterone connection makes vitamin D particularly relevant after 50. The gradual decline in testosterone that begins in the mid-30s and accelerates through the 50s and 60s is influenced by multiple factors — and vitamin D status is increasingly recognized as one of them. Research has consistently found lower testosterone levels in vitamin D-deficient men and meaningful improvements following correction of deficiency.
There is also evidence connecting adequate vitamin D levels to prostate health. Vitamin D receptors are highly expressed in prostate tissue, and observational data links deficiency with increased risk of prostate enlargement and prostate cancer progression. While this evidence does not yet support supplementation as a clinical intervention for prostate conditions, maintaining optimal vitamin D levels as a foundational aspect of men’s health over 50 is well-supported by the available data.
People with Limited Sun Exposure or Darker Skin Tone
As discussed in the sunshine paradox section, these two groups face the most consistent structural barriers to maintaining adequate vitamin D through natural means. Supplementation is not a workaround for these individuals — it is a straightforward nutritional necessity that closes a gap the environment does not allow them to fill through sun exposure alone.
Anyone in the “Sufficient But Not Optimal” Range
Perhaps the most overlooked group is people with serum levels between 20 and 30 ng/mL — technically sufficient by conventional standards but below what growing research suggests is the functional optimum for non-skeletal benefits. These individuals will not be flagged as deficient on a routine blood test. Their doctor may not mention vitamin D at all. And yet they may be missing meaningful benefit in immune function, mood regulation, and hormonal health that modest supplementation could provide.
Vitamin D3 Benefits in Modern Supplements
Most high-quality multi-ingredient supplements that target male health, immune function, or overall vitality now include vitamin D3 as a core component — and for good reason. In a well-designed formula, vitamin D3 does not just fill a nutritional gap; it amplifies the function of the other ingredients working alongside it.

ProstaVive: Vitamin D in a Complete Male Health Formula
ProstaVive is a powdered supplement formulated specifically for male health, combining vitamin D3 with a range of botanicals and minerals — including zinc, magnesium, tongkat ali, and nettle root — that target prostate function, hormonal balance, and urinary comfort. The inclusion of vitamin D3 in this formula reflects what the research supports: adequate vitamin D is not peripheral to male hormonal health, it is structural to it. Vitamin D deficiency in men is independently associated with lower testosterone, reduced immune modulation in prostate tissue, and compromised mineral metabolism.

For anyone looking to understand how ProstaVive positions vitamin D3 within a broader male health protocol, you can read our complete review at healthyroutinelab.com/prostavive-review.
Spartamax: Vitamin D Paired with Testosterone and Vitality Support
Spartamax is a male vitality formula delivered in gummy form, combining vitamin D3 with ingredients like tongkat ali, ashwagandha, maca root, and zinc — a stack designed to support energy, stamina, hormonal function, and circulation. The vitamin D3 inclusion here serves a specific purpose: zinc and vitamin D work synergistically in testosterone synthesis pathways, and both are commonly suboptimal in men over 40 who are not actively monitoring their levels. Spartamax addresses that gap within a formula built for daily use and long-term consistency.

For a detailed breakdown of Spartamax’s full formula, ingredients, and how it fits into a male vitality routine, see our full review at healthyroutinelab.com/spartamax-review.
How Long Does Vitamin D Take to Work?
This is one of the most searched questions about vitamin D supplementation — and the honest answer depends heavily on what outcome you are measuring and what your starting level is.
For raising serum 25-hydroxyvitamin D levels, the timeline is relatively well-characterized. At a standard supplementation dose of 1,000–2,000 IU daily, it typically takes 6 to 8 weeks to reach a new steady-state level. Reaching that plateau requires time because vitamin D accumulates gradually in tissue stores. Higher doses accelerate the rise but should not be used without baseline testing and medical guidance.
For functional outcomes, the timelines are longer and more variable. Studies examining the effect of vitamin D supplementation on immune function, mood, and energy generally run for 3 to 6 months before measuring outcomes — reflecting the time required not just to raise blood levels but for downstream biological effects to manifest. The 2018 sleep RCT referenced earlier showed improvements at 8 weeks; depression studies typically run 12 weeks or more. Testosterone studies have used 12-month protocols.
A few important caveats. If you begin supplementation with a severely low baseline — below 12 ng/mL — the timeline to functional benefit may be longer, and a higher initial loading dose under medical supervision may be warranted. If your baseline is already in the sufficient range (above 30 ng/mL), the incremental benefit of additional supplementation is likely to be modest and may take longer to detect, if it is detectable at all.
The practical guidance: get tested before supplementing if possible. Know your baseline. Retest after 8–12 weeks at your chosen dose. And give the process several months before drawing conclusions about whether it is working — the outcomes you care most about are downstream of blood level changes, not simultaneous with them.
Vitamin D Dosage, Timing, and Safety
How Much Vitamin D Should You Take Daily?

This is where official recommendations and research-based practice diverge most visibly, and it is worth being transparent about that tension.
The current US Recommended Dietary Allowance (RDA) is 600 IU per day for adults up to age 70, and 800 IU for those over 70. These figures were established primarily to prevent rickets and maintain bone mineralization — not to optimize the non-skeletal benefits that have emerged from more recent research.
Many researchers and clinicians who work specifically in vitamin D argue that these figures are too conservative for most adults. The large VITAL trial used 2,000 IU daily as its supplementation dose. The 2025 evidence review published in Nutrients by Grant et al. — the most-cited vitamin D paper of that year — recommended daily intakes of 2,000–4,000 IU to reach serum levels associated with meaningful risk reduction across multiple outcomes.
A practical middle ground for most healthy adults not at risk of toxicity: 1,000–2,000 IU of vitamin D3 daily is a reasonable maintenance dose that is well within safe limits and consistent with the dosing used in the majority of positive clinical trials. Individuals with confirmed deficiency, those over 60, or those with conditions that impair absorption may need higher doses — determined by testing, not guesswork.
Best Time to Take Vitamin D
Vitamin D is fat-soluble, which means absorption is significantly enhanced when taken with a meal containing dietary fat. A study published in the Journal of Bone and Mineral Research found that taking vitamin D with the largest meal of the day increased absorption by approximately 50% compared to taking it on an empty stomach.
There is no strong evidence that time of day matters independently — morning versus evening supplementation does not appear to meaningfully affect serum levels. The priority is consistency and fat co-ingestion, not clock timing.
Vitamin D with K2: Why the Combination Matters
Vitamin K2 has emerged as an important companion to vitamin D in supplementation protocols, and the reasoning is biologically grounded. Vitamin D increases intestinal calcium absorption — which is the point. But calcium needs to be directed into bone and teeth rather than soft tissues and arterial walls. Vitamin K2 activates two proteins critical to this routing: osteocalcin, which incorporates calcium into bone matrix, and matrix GLA protein (MGP), which inhibits calcium deposition in arteries.
In populations consuming diets very low in vitamin K2 — which describes most Western diets, where fermented foods and certain organ meats that provide K2 are largely absent — high-dose vitamin D supplementation without K2 may theoretically increase soft tissue calcification risk. The evidence for this concern in healthy adults at typical supplementation doses is not definitive, but the biological rationale is strong enough that many nutrition researchers recommend taking D3 and K2 together, particularly at doses above 2,000 IU.
Can You Take Too Much Vitamin D?
Yes — and this is a real risk worth taking seriously, even if it is significantly rarer than vitamin D deficiency.
Vitamin D toxicity (hypervitaminosis D) results from excessive supplementation over time — not from sun exposure, which is self-limiting through skin feedback mechanisms. The tolerable upper intake level established by the National Academy of Medicine is 4,000 IU per day for adults. Toxicity typically appears at sustained intakes well above this — usually 10,000 IU or more daily for extended periods.
The primary mechanism of toxicity is hypercalcemia — elevated blood calcium — which can cause nausea, weakness, frequent urination, kidney stones, and in severe cases, cardiac arrhythmias. A 2024 ConsumerLab analysis found several vitamin D supplements on the market containing significantly more than their labeled dose — a reminder that supplement quality control matters.
The practical guardrail is simple: if you are supplementing at 1,000–2,000 IU daily, you are well within safe parameters. If you are using higher doses — particularly 5,000 IU or above — periodic blood testing for both 25-hydroxyvitamin D and serum calcium is a reasonable precaution.
Frequently Asked Questions About Vitamin D Benefits
What are the signs of vitamin D deficiency in adults?
The most common signs include persistent fatigue that does not improve with rest, diffuse bone or muscle aching, frequent respiratory infections, low mood or seasonal depression, and impaired wound healing. Many people with moderate deficiency are asymptomatic, which is why a blood test is the only reliable way to confirm status. Hair thinning and brain fog are less commonly discussed but are also reported in individuals with low serum levels.
How long does it take for vitamin D supplements to raise levels?
At typical supplementation doses of 1,000–2,000 IU daily, serum 25-hydroxyvitamin D levels generally reach a new plateau within 6 to 8 weeks. Functional outcomes — mood, energy, immune response — often take longer to manifest, typically 3 to 6 months. Starting from a lower baseline and using higher doses (under medical supervision) can accelerate the process.
Is vitamin D3 better than vitamin D2?
For most purposes, yes. Vitamin D3 raises and sustains serum levels more effectively than D2, and it is the form the body produces naturally through sun exposure. D2 is plant-derived and may be preferred by those following a strict vegan diet — vegan vitamin D3 sourced from lichen is also available and performs comparably to animal-derived D3.
Can vitamin D deficiency cause hair loss?
The evidence is observational, but biologically plausible. Vitamin D receptors are expressed in hair follicle cells and play a role in the hair growth cycle. Low vitamin D has been associated with alopecia areata and diffuse hair shedding in multiple studies. Correcting deficiency in affected individuals has shown improvements in some research, though supplementation is not yet established as a primary treatment for hair loss.
Does vitamin D help with depression and anxiety?
The strongest evidence supports vitamin D’s role in improving depressive symptoms in individuals with clinically diagnosed depression who also have low vitamin D levels. Meta-analyses of randomized trials show meaningful effects in this specific population. The evidence for anxiety is less developed. Supplementing vitamin D when levels are already sufficient is unlikely to produce significant mood effects.
How can I raise my vitamin D levels fast?
The most effective approach is a higher-dose supplementation protocol under medical guidance — often 4,000–10,000 IU daily for a defined period to correct a confirmed deficiency, followed by a maintenance dose. Getting tested first is essential: without knowing your baseline, you cannot accurately dose or track progress. Retest after 8 weeks. Sun exposure during peak UVB hours with significant skin exposure can contribute meaningfully in summer months, but is rarely sufficient on its own to correct established deficiency.
How long should I stay in the sun to get enough vitamin D?
It depends on several factors: skin tone, time of day, season, geographic latitude, and amount of skin exposed. A rough guideline for a fair-skinned adult in summer at mid-latitudes: 10–15 minutes of midday sun exposure on arms and legs may produce 1,000–3,000 IU of vitamin D. Darker skin tones require significantly more time. Above approximately 35 degrees latitude, meaningful synthesis is not possible in winter months regardless of sun time. These variables make sun exposure an unreliable standalone strategy for most people across all seasons.
What is the difference between vitamin D and vitamin D3?
“Vitamin D” is the general term for the family of related compounds — including D2 and D3. “Vitamin D3” refers specifically to cholecalciferol, the form produced in human skin and found in animal-based foods. It is the most bioavailable and biologically active form for supplementation. When you see “vitamin D3” on a supplement label, it tells you specifically which form you are getting — and D3 is the preferred form for raising and sustaining blood levels.
The Bottom Line
Vitamin D benefits extend well beyond bone health — and the evidence supporting its role in immune function, mood regulation, testosterone, sleep, cardiovascular health, and inflammation is more robust than most people realize. But the critical insight that most content misses is this: the question is not simply whether you are deficient. It is whether your levels are genuinely optimized for the full range of biological functions that vitamin D governs.
Sitting at 22 ng/mL may keep you out of the clinical deficiency category. It does not mean vitamin D is doing its job. The research increasingly points to a functional optimum somewhere between 30 and 50 ng/mL — a range that requires deliberate effort to reach and maintain for a significant portion of adults, particularly those over 50.
The practical steps are straightforward: get tested, supplement with vitamin D3 at a dose appropriate for your baseline, take it with a fatty meal for maximum absorption, and consider pairing it with K2 at higher doses. Give it 8 to 12 weeks before retesting. And recognize that the functional benefits you are after — better immunity, more stable mood, stronger sleep, and healthier hormone levels — take longer to manifest than the serum level changes that precede them.
Vitamin D benefits are real and well-documented. Getting them requires more than occasionally topping up your levels. It requires treating this hormone with the seriousness its biology demands.
Disclaimer: This content is for informational and educational purposes only and does not constitute medical advice. Vitamin D supplementation, particularly at higher doses, should be discussed with a qualified healthcare provider. Do not use this information to self-diagnose or treat any health condition.








