Most articles about l-arginine benefits start the same way: amino acid, nitric oxide, blood flow, better pumps. The information is technically correct. It is also deeply incomplete — and that gap is exactly why so many people supplement with l-arginine, feel nothing, and conclude the ingredient doesn’t work.
The real story is more interesting. L-arginine is one of the most clinically studied amino acids in human nutrition, with documented effects on erectile function, blood pressure, cardiovascular health, immune defense, and metabolic markers. But it works through a mechanism that has a ceiling — and that ceiling depends almost entirely on the health of your blood vessels, not on how much you take. Understanding that distinction changes how you evaluate this ingredient, who actually benefits from supplementing it, and why the research looks so inconsistent across different populations.
This post covers the science without the hype.
What Is L-Arginine?
L-arginine is a semi-essential amino acid — a classification that trips people up more than it should. Semi-essential means the body can synthesize it on its own from other amino acids, primarily from citrulline via the kidneys, but production doesn’t always meet demand. During periods of rapid growth, illness, injury, significant physical stress, or advancing age, the body’s internal production falls short. Dietary intake and supplementation fill the gap.
The “L” prefix is a chemistry designation indicating the levorotatory form — the molecular orientation that mirrors the amino acids the human body naturally produces and uses. This is the form found in food proteins and in virtually all commercial supplements.
L-arginine is involved in protein synthesis, but that is not the reason it has attracted so much research attention. Its primary claim to clinical relevance is its role as the direct precursor to nitric oxide (NO) — a signaling molecule that controls how blood vessels expand and contract, regulates blood pressure, governs blood flow to tissues and organs, and plays a central role in immune defense and cellular communication.
The Active Compound: How Arginine Becomes Nitric Oxide
The conversion is direct. The enzyme nitric oxide synthase (NOS) — specifically endothelial NOS (eNOS) in the lining of blood vessels — uses l-arginine as its substrate and converts it into nitric oxide and l-citrulline as a byproduct. The nitric oxide then diffuses into surrounding smooth muscle cells, activates guanylate cyclase, raises cyclic GMP (cGMP) levels, and causes those muscles to relax. The blood vessel widens. Blood flows more freely.
That chain of events — arginine → eNOS → NO → vasodilation — is the core of nearly every l-arginine benefit that has meaningful clinical evidence behind it. Blood pressure reduction, improved erectile function, better circulation to peripheral tissues, enhanced oxygen delivery during exercise: all of them run through this pathway.
What most content doesn’t explain is that the pathway has a ceiling. When eNOS is already saturated with arginine — which is the baseline state in healthy adults — adding more arginine does not produce more nitric oxide. The enzyme is already running at capacity. The paradox becomes relevant in the next section.
L-Arginine Forms and Supplement Types: HCl, AKG, and Free-Form
Three forms dominate the supplement market. L-Arginine HCl (hydrochloride) is the most common, most studied, and most affordable. It delivers a high percentage of elemental arginine per gram and is the form used in virtually all clinical trials measuring blood pressure and erectile function outcomes.
L-Arginine AKG (alpha-ketoglutarate) combines arginine with a Krebs cycle intermediate, theoretically improving cellular uptake. It appears frequently in pre-workout formulas. The bioavailability advantage over standard HCl remains unproven in rigorous head-to-head trials.
Free-form arginine is the base amino acid without a salt carrier. It is absorbed similarly to HCl but is less stable in powder form. For most practical purposes — and for understanding the clinical evidence — l-arginine HCl is the reference standard. When a study cites 3g or 6g of arginine, it is almost always HCl unless stated otherwise.
Natural Food Sources of L-Arginine
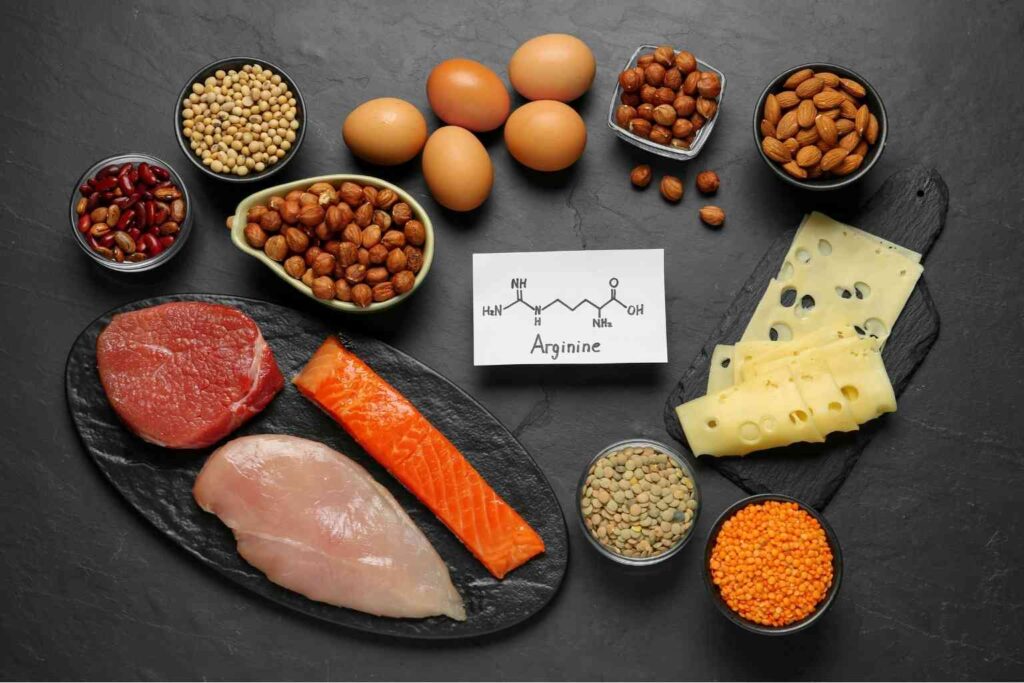
The body obtains l-arginine from dietary protein, and the range across common foods is wide enough to matter. Pumpkin seeds are the densest source per calorie — a one-ounce serving delivers roughly 2.5g of arginine, a figure that exceeds most other plant foods by a significant margin. Turkey and chicken breast provide approximately 2–2.5g per 100g of cooked meat. Pork loin, lean beef, and salmon fall in a similar range. Soybeans, peanuts, chickpeas, and lentils are meaningful plant sources, particularly relevant for people limiting animal protein intake.
The practical takeaway is that most adults eating adequate protein from varied sources are likely consuming 4–6g of dietary arginine per day. That level of intake keeps baseline plasma arginine adequate for normal physiological function. It does not, however, necessarily restore arginine availability in a compromised endothelium — which is the clinical context where supplementation becomes relevant.
Turkey, Pumpkin Seeds, and Watermelon: Why These Three Stand Out
Turkey is worth highlighting because it is one of the few commonly consumed foods that consistently delivers high arginine per serving alongside a low arginine-to-lysine ratio, which matters for people managing certain amino acid sensitivities. Pumpkin seeds stand out for plant-based eaters because two tablespoons provide more arginine than most protein bars while also delivering magnesium and zinc — two minerals that support the same vascular pathways as nitric oxide.
Watermelon deserves its own mention for a different reason. The fruit is rich in L-citrulline, not arginine directly — but citrulline is converted to arginine in the kidneys via the argininosuccinate pathway, which is the same route the body uses to produce its own arginine internally. This means that eating watermelon increases plasma arginine levels through a back-door mechanism that largely bypasses the intestinal degradation problem that limits oral arginine supplements. The watermelon-citrulline-arginine connection explains why the fruit appears in both arginine-focused and citrulline-focused nutritional literature and why researchers studying nitric oxide-supporting diets consistently include it.
How Does L-Arginine Work? The Mechanisms Behind the Benefits
The nitric oxide pathway is the primary mechanism, but it is not the only one. Five mechanisms account for the majority of l-arginine’s documented effects.
Endothelial nitric oxide production via eNOS activation is the headline mechanism — covered above. When functioning correctly in a compromised endothelium, this is responsible for blood pressure reduction, vascular dilation, and improved blood flow to target tissues including penile erectile tissue.
Insulin secretion stimulation is a separate, distinct mechanism. L-arginine is a potent stimulus for pancreatic beta-cell insulin release, independent of blood glucose levels. This is why arginine is used clinically as a diagnostic challenge for beta-cell function and why it appears in research on glucose metabolism and insulin sensitivity improvement.
Urea cycle participation is the arginine mechanism that most supplement content ignores entirely. Arginine is the direct precursor to ornithine and urea in the liver — the pathway that clears ammonia from the bloodstream after protein metabolism. In high-protein diets or intense training, adequate arginine availability supports more efficient nitrogen clearance.
Immune cell modulation operates through arginine’s role in lymphocyte T-cell proliferation and macrophage activity. Immune cells — especially macrophages — produce nitric oxide in large quantities as part of pathogen defense, and they compete with endothelial cells for available arginine under conditions of physiological stress. This competition is one reason arginine depletion correlates with immune suppression in post-surgical and critically ill patients.
Polyamine synthesis is the fifth mechanism. Arginine is converted via ornithine to putrescine, spermidine, and spermine — polyamines that stabilize DNA structure and regulate cell division. This pathway is the basis for l-arginine’s documented role in wound healing and tissue repair contexts, and also the mechanistic foundation for research on arginine in reproductive health.
L-Arginine Benefits: What the Research Actually Shows
The evidence base for l-arginine benefits is uneven by design — strong in some areas, preliminary in others, and genuinely absent in a few places where marketing claims run ahead of the science. What follows is calibrated to match each benefit to the actual quality and consistency of the evidence supporting it.
1. Erectile Function: The Clearest Clinical Signal
A 2022 multicenter, double-blind, randomized, placebo-controlled trial published in International Urology and Nephrology enrolled 98 men with vasculogenic erectile dysfunction and administered 6g of oral l-arginine daily for 90 days. The results were clinically meaningful: IIEF-6 scores increased significantly across the full cohort, and penile peak systolic flow velocity on duplex ultrasonography improved in men with mild-to-moderate vasculogenic ED. Men with severe vasculogenic ED showed improvement in functional scores but not in vascular flow metrics — a distinction that matters enormously for setting realistic expectations.

Earlier meta-analyses paint a consistent picture. A 2019 systematic review and meta-analysis in The Journal of Sexual Medicine examined 10 studies and found that dosages between 1,500 and 5,000mg daily produced significant improvements in mild-to-moderate ED compared to placebo, alongside higher scores of sexual satisfaction.
The mechanism is direct: erectile tissue depends on nitric oxide-mediated relaxation of cavernosal smooth muscle, which allows blood to rush into the corpora cavernosa and sustain an erection. When eNOS activity is suboptimal — due to age, endothelial dysfunction, or vascular compromise — restoring substrate availability improves the signal. This is one of the two areas where l-arginine benefits have the most robust human clinical evidence.
2. Blood Pressure: Consistent Effect, Dose-Dependent Response
A 2022 systematic review and dose-response meta-analysis in Advances in Nutrition examined 30+ randomized controlled trials and confirmed that oral l-arginine supplementation produces statistically significant reductions in both systolic and diastolic blood pressure. The effect was more pronounced in systolic readings and in participants with baseline hypertension compared to normotensive individuals.

The dose-response relationship is real. Studies using doses below 3g daily showed smaller and less consistent effects. Doses of 6g or more — particularly in hypertensive populations — showed the most reliable reductions. A 2025 systematic review in Human Nutrition and Metabolism confirmed that doses at or above 8g daily improved lipid profiles and liver enzyme markers alongside blood pressure, suggesting broader cardiometabolic benefit at higher therapeutic doses.
Blood pressure reduction via arginine is mechanistically clean: more NO in the endothelium → more vasodilation → lower peripheral resistance → lower pressure. It is one of the most direct demonstrations of the pathway in action.
3. Blood Flow and Cardiovascular Support
The evidence for peripheral arterial disease (PAD) is instructive because it shows both the promise and the limits of l-arginine supplementation. Short-term oral or intravenous arginine — up to 8 weeks — increases blood flow in people with PAD and produces measurable improvements in endothelium-dependent vasodilation, according to multiple RCTs and reviews cited by Mayo Clinic. Use beyond 6 months, however, does not appear to improve walking speed or distance in PAD patients, and one long-term cardiac study raised concerns about arginine supplementation in post-myocardial infarction patients.
For adults with mild-to-moderate endothelial dysfunction who are not in a post-cardiac event context, the blood flow evidence is positive and consistent within the short-to-medium timeframe. The pattern holds for angina as well — multiple studies have shown reduced symptom frequency and improved exercise tolerance in people with mild angina taking oral arginine.
4. Exercise Performance: Real Benefits With Important Caveats
A 2020 review and meta-analysis in Nutrients confirmed that l-arginine supplementation taken 60 to 90 minutes prior to exercise produces measurable improvements in both aerobic and anaerobic performance markers. The effect size is real but modest, and it diminishes with longer supplementation windows — suggesting that acute dosing before activity is more effective than chronic background dosing for performance purposes.

The important caveat: the same meta-analysis found that l-citrulline outperformed l-arginine for exercise performance outcomes in most direct comparisons. The reason is bioavailability. Oral l-arginine is significantly degraded by arginase enzymes in the gut and liver before it reaches the bloodstream, limiting how much actually arrives at the endothelium. L-citrulline bypasses this degradation and raises plasma arginine more effectively per gram consumed. For pure performance purposes, citrulline has the edge. For people using arginine in a broader health context — blood pressure, erectile function, cardiovascular support — the bioavailability limitation is still manageable at appropriate doses.
5. Blood Sugar and Metabolic Support
A 2017 study in middle-aged adults with metabolic syndrome and impaired glucose tolerance found that l-arginine supplementation delayed the onset of type 2 diabetes over a follow-up period of several years. The mechanism involves both direct insulin secretion stimulation from pancreatic beta cells and arginine’s role in improving insulin sensitivity at the cellular level.

A 2025 proof-of-principle RCT in Human Nutrition and Metabolism — 60 obese individuals over 8 weeks — found that a combination of l-arginine, l-citrulline, and micronutrients significantly reduced elevated triglyceride levels and improved metabolic syndrome severity scores. These are preliminary findings from a single study with a small sample, but the mechanistic rationale is sound.
This is an area of genuine scientific interest with promising early data. It does not yet warrant the confidence level of the blood pressure or ED evidence.
6. Immune Function and Wound Recovery
L-arginine’s immune role operates through two distinct pathways. Macrophages use arginine to produce nitric oxide as a direct antimicrobial weapon — and in settings of acute infection or post-surgical recovery, arginine demand by immune cells rises sharply. Clinical nutrition guidelines in critical care have for decades included arginine-enriched enteral formulas specifically because of this demand, with documented reductions in infection complications and faster tissue recovery in surgical populations.
The wound healing connection is mechanistically linked: arginine-derived polyamines support collagen synthesis and cell proliferation. The evidence in healthy adults without surgical or injury context is much thinner — supplementing arginine for general “immune support” in an otherwise healthy person has limited clinical backing. But in the context of recovery from injury, surgery, or significant physical stress, the rationale is solid.
7. Pregnancy and Preeclampsia: An Underreported Application
A 2025 systematic review and meta-analysis published in BJOG: An International Journal of Obstetrics and Gynaecology — 20 RCTs, 2,028 women — found that l-arginine supplementation reduced the incidence of preeclampsia and related hypertensive outcomes in pregnancy. The effect was documented for both prevention and treatment contexts, though the authors noted that optimal timing of initiation and target populations require further research.

The mechanism is straightforward: preeclampsia involves endothelial dysfunction and impaired nitric oxide production in placental vasculature. Restoring substrate availability supports NO production in a context where the endothelium is demonstrably compromised — which is precisely the condition where arginine supplementation is most effective.
This application is almost entirely absent from mainstream supplement content about l-arginine benefits. It is one of the more clinically substantiated uses of the amino acid.
The L-Arginine Paradox: Why It Works Better When Your Body Is Under Stress
Here is the finding that changes how you should think about l-arginine: in healthy adults with normal endothelial function, plasma arginine is already well above the concentration needed to saturate eNOS. The enzyme is running at full capacity. Adding more arginine — by eating more protein or by taking a supplement — does not increase nitric oxide production because substrate availability is not the limiting factor. The ceiling is already reached.
This is documented. A review published in PMC (National Library of Medicine) states directly that normal, non-elevated l-arginine levels in the blood are already high enough to saturate endothelial NOS, and therefore supplementation in healthy individuals will not enhance NO production because arginine is not rate-limiting for eNOS.
The picture changes completely when the endothelium is compromised. In hypertension, the endothelium accumulates ADMA (asymmetric dimethylarginine) — an endogenous inhibitor of eNOS that competes with arginine for enzyme binding. Higher ADMA levels effectively shift the arginine-to-ADMA ratio, making arginine functionally deficient even when absolute plasma levels are normal. In this context, supplemental arginine competes against ADMA and restores NO production that would otherwise be suppressed.
In aging, eNOS expression declines and oxidative stress degrades nitric oxide before it can act. In insulin resistance and metabolic syndrome, endothelial dysfunction follows a similar pattern. In atherosclerosis, ADMA accumulates further. Across all of these conditions — which are extremely common in adults over 45 — the arginine-to-ADMA ratio becomes the clinically relevant variable, not absolute arginine levels alone.
This is why the clinical trial data on l-arginine benefits is so consistent in hypertensive patients, adults with vasculogenic ED, and people with metabolic syndrome — and so mixed in young, healthy, athletic populations. The paradox is not a flaw in the evidence. It is the evidence telling you exactly who this amino acid is actually for.
L-Arginine vs. L-Citrulline: Which One Should You Actually Take?
The comparison matters practically, and the answer is not as simple as “citrulline is better.”

When you take oral l-arginine, a significant portion is broken down by arginase enzymes in the small intestine and liver before it reaches systemic circulation. This pre-systemic metabolism — called first-pass degradation — reduces the amount of arginine that actually arrives at the endothelium where it needs to work. At standard supplement doses of 500mg to 2g, the degradation is substantial enough to meaningfully limit the effect.
L-citrulline bypasses this problem entirely. Citrulline is not a substrate for intestinal arginase. It passes through the gut intact, is converted to arginine in the kidneys via the argininosuccinate pathway, and delivers a sustained, higher plasma arginine level than an equivalent oral dose of arginine itself. Multiple head-to-head comparisons have confirmed this: gram for gram, citrulline raises plasma arginine more effectively than arginine does.
So why would anyone choose l-arginine? Three reasons. First, at higher doses — 3g to 6g and above — enough arginine survives first-pass degradation to produce clinically meaningful effects, as demonstrated in the ED and blood pressure RCTs. Second, l-arginine is less expensive per gram than citrulline, which matters when therapeutic doses are required over extended periods. Third, for specific clinical contexts — particularly the arginine-pycnogenol combination studied in ED research — l-arginine was the form used in the trials that generated the evidence, and substituting citrulline for arginine in those protocols has not been equivalently validated.
The practical framework: for exercise performance and general nitric oxide support in healthy adults, citrulline is the more efficient choice. For therapeutic use in adults with confirmed hypertension, vasculogenic ED, or other endothelial dysfunction contexts, l-arginine at 3–6g daily has the clinical evidence behind it and remains a legitimate first choice — particularly when cost over months of use is a consideration.
Who Benefits Most from L-Arginine?
The paradox framework makes the answer to this question unusually precise.
Men between 45 and 65 with mild-to-moderate vasculogenic erectile dysfunction are the population with the clearest evidence base. Endothelial dysfunction is the dominant mechanism of ED in this demographic, ADMA accumulation is documented with advancing age, and the clinical trials showing significant IIEF-6 improvement were conducted specifically in this population. This is where the evidence is strongest and most actionable.
Adults with prehypertension or stage 1 hypertension — systolic 120–139 or diastolic 80–89 — represent the second clearest application. Blood pressure reduction in this range using 3–6g of arginine daily has been demonstrated across multiple RCTs, with the benefit appearing within 4–8 weeks of consistent use.
Adults with metabolic syndrome or impaired glucose tolerance are a third meaningful group, based on the mechanistic alignment between arginine’s insulin secretion effects and the metabolic dysfunction pattern in this population. The evidence here is earlier-stage but mechanistically well-grounded.
Athletes in masters categories — typically 40 and above — who are experiencing reduced training recovery and lower nitric oxide-mediated blood flow face a context that resembles early endothelial compromise more than it resembles the healthy young athlete population where arginine tends to show limited effect. For this group, arginine’s performance benefits are more likely to manifest than in younger, healthy counterparts.
People in recovery from surgery, injury, or significant physical illness represent the final high-benefit population — one that is often overlooked in supplement marketing but has the most extensive clinical nutrition evidence behind arginine use.
L-Arginine for Men Over 50: Where the Evidence Is Strongest
By age 40, nitric oxide production has declined by roughly 50% compared to peak levels in young adulthood — a figure cited consistently across vascular aging research. By 50, the decline is compounded by accumulating ADMA, declining eNOS expression, and increasing oxidative stress that degrades NO before it can act. These changes are not abstractions. They manifest as reduced exercise tolerance, elevated resting blood pressure, slower post-exercise recovery, and — in many men — the onset of vasculogenic erectile dysfunction.

This is the population for which l-arginine supplementation is most supported by clinical evidence. The RCTs that show meaningful effects on blood pressure, erectile function, and vascular markers are populated predominantly by adults over 45 with some degree of established endothelial compromise. Younger, healthier adults see smaller and less consistent effects precisely because their eNOS is not yet operating in the arginine-limited zone.
L-Arginine in Modern Supplements
Because l-arginine’s primary mechanism runs through nitric oxide production, the most defensible supplement formulas are those that support the NO pathway from multiple angles simultaneously — rather than relying on arginine alone at doses that may not survive first-pass degradation.
Spartamax — L-Arginine Combined with Blood Flow Co-Factors
Spartamax is a daily male performance gummy that combines l-arginine with beet root and grape seed extract — a formulation choice that reflects a genuine understanding of how nitric oxide production works. L-arginine supports the arginine-eNOS-NO pathway. Beet root delivers dietary nitrates, which the body converts to nitric oxide via a separate, nitrate-nitrite-NO pathway that does not require eNOS at all.
Grape seed extract provides oligomeric proanthocyanidins (OPCs), which have documented effects on endothelial function and support eNOS activity through antioxidant mechanisms that reduce oxidative nitric oxide degradation.

The formula also includes Tongkat Ali, Maca Root, Ashwagandha, and Horny Goat Weed — addressing the hormonal and adaptogenic dimensions of male sexual performance that run parallel to, but distinct from, the vascular mechanism that arginine targets. For men whose performance concerns span both blood flow and drive, that multi-mechanism approach is more complete than a single-ingredient arginine product.
For readers who want a full breakdown of the formula, dosages, clinical context, and what to realistically expect, the detailed analysis is available here: Read the full Spartamax review here.
How Long Does L-Arginine Take to Work?
The answer depends entirely on what outcome you are looking for, because the timelines for acute effects and chronic effects are very different.

Acute vasodilation — the kind relevant to pre-workout blood flow and short-term blood pressure reduction after a dose — occurs within 60 to 90 minutes of ingestion. This is the window most consistently cited in exercise performance research for timing arginine supplementation before activity.
Chronic effects on erectile function and blood pressure operate on a longer timeline. The multicenter RCT that showed significant IIEF-6 score improvement ran for 90 days. Blood pressure meta-analyses show consistent effects emerging at 4 to 8 weeks of daily supplementation. Endothelial function improvements, assessed by flow-mediated dilation, require consistent daily dosing for at least 4 weeks before changes are measurable.
The practical implication: if you try l-arginine for two weeks and notice nothing, you have not given the mechanism the time it needs to produce chronic structural benefits. If you are using it acutely before exercise, the window matters — taking it an hour before activity captures the peak plasma elevation window.
L-Arginine Dosage, Timing, and Safety
Dosage: What the Research Uses vs. What Supplements Deliver
There is a meaningful gap between the doses used in clinical trials and the doses found in most commercial supplements. Standard over-the-counter capsules typically deliver 500mg to 1g per serving. The doses used in RCTs showing significant erectile function improvement range from 2.5g to 6g daily. The doses used in blood pressure meta-analyses showing consistent effects start at approximately 3g and show stronger results at 6g and above. Metabolic syndrome trials using both arginine and citrulline have used doses of 8g total and above.
This gap matters. At 500mg to 1g daily, a meaningful portion of the dose is degraded before reaching systemic circulation, and the remaining amount may not be sufficient to shift the arginine-to-ADMA ratio in compromised endothelium. For therapeutic intent — ED, blood pressure, cardiovascular support — doses of 3g to 6g daily are supported by clinical evidence. For general supplementation or pre-workout use, 2–3g taken 60–90 minutes before activity is reasonable.
Divided dosing — two to three smaller doses across the day rather than one large bolus — reduces gastrointestinal side effects and may maintain more consistent plasma levels, particularly at higher total daily doses.
Safety and Side Effects: What to Watch For
Oral l-arginine is generally well-tolerated in healthy adults. The National Institutes of Health indicates that doses up to 9g per day are considered safe for short-term use of several weeks. The most common side effect is gastrointestinal discomfort — bloating, loose stools, or nausea — which tends to appear at higher single doses and can usually be managed by dividing the daily intake across multiple smaller doses.
Blood pressure reduction is a known pharmacological effect. For most people managing hypertension, this is the intended outcome. For people with already-low blood pressure or those taking antihypertensive medications, additive hypotensive effects warrant monitoring and a conversation with a physician before supplementing.
L-arginine can worsen herpes outbreaks in people with herpes simplex virus. Arginine facilitates herpes replication, and in individuals with known HSV, high-dose arginine supplementation can trigger recurrences. Pairing with lysine — which competitively inhibits arginine uptake — is sometimes used to mitigate this, though that approach has its own tradeoffs worth discussing with a healthcare provider.
Interactions and Precautions: The Contraindication Most People Miss
There is a safety signal that is almost entirely absent from mainstream supplement content, and it needs to be stated clearly. A randomized clinical trial published in JAMA in 2006 — the VINTAGE MI trial — was halted early because patients who had recently experienced a myocardial infarction and were randomized to l-arginine supplementation showed significantly higher mortality than the placebo group. The mechanism is not fully established, but the finding is serious enough that Mayo Clinic, WebMD, and the NIH all explicitly state that l-arginine should not be taken by people who have had a recent heart attack.
This is not a minor caveat buried in fine print. It is an active contraindication with clinical mortality data behind it. People with recent cardiac events, unstable heart disease, or severe cardiovascular compromise should not use l-arginine supplementation without direct physician guidance.
L-arginine also interacts with nitrate medications (nitroglycerin), sildenafil and other PDE5 inhibitors, blood pressure medications including potassium-sparing diuretics, and blood thinners. In each case, the risk is additive hypotension or altered pharmacokinetics. Anyone managing cardiovascular conditions or taking medications in these classes should consult a physician before adding l-arginine.
Frequently Asked Questions About L-Arginine
Does l-arginine increase testosterone?
Not directly. L-arginine does not act on the hypothalamic-pituitary-gonadal axis and has no documented testosterone-stimulating mechanism. Some early studies showed a transient increase in growth hormone secretion with high-dose intravenous arginine, but oral supplementation at realistic doses does not replicate this effect reliably. The 2022 vasculogenic ED trial noted a non-significant trend toward higher total testosterone in the l-arginine group — but “non-significant trend” is exactly what the words suggest: not a proven effect. If testosterone support is the goal, arginine is not the right tool for that job.
Can I take l-arginine before bed or should I take it in the morning?
For blood pressure and chronic endothelial support, timing is less critical — consistent daily intake matters more than the specific hour. For erectile function support, some evidence suggests that taking arginine earlier in the day allows peak plasma levels to coincide with periods of likely sexual activity. For exercise performance, 60 to 90 minutes before training is the evidence-based window. Taking arginine on an empty stomach improves absorption; taking it with a high-protein meal slows uptake slightly because dietary amino acids compete for intestinal transporters.
What is the right l-arginine dosage for erectile dysfunction?
The clinical evidence supports 2.5g to 6g daily, in divided doses, for at least 4 to 8 weeks before assessing response. The 2022 multicenter RCT used 6g daily for 90 days as its protocol. The 2019 meta-analysis found significant improvements across studies using 1.5g to 5g daily, with larger effects at higher doses. Starting at 3g daily — split into two 1.5g doses — and assessing after 8 weeks is a reasonable starting point before adjusting upward if needed.
Is l-arginine safe for long-term use?
The honest answer is that long-term safety data in humans is limited. Short-term safety at doses up to 9g daily for several weeks is well-established. Long-term safety beyond 3 to 6 months has not been as rigorously characterized in large human trials. Animal studies suggest good tolerability at doses far exceeding typical human supplementation. The most clinically conservative approach for extended use — particularly above 3g daily — is periodic reassessment with a physician, especially for people on blood pressure or cardiovascular medications.
Does l-arginine work for men over 60?
The evidence supports it, with realistic calibration. In men over 60 with mild-to-moderate vasculogenic erectile dysfunction, the mechanistic conditions that make arginine supplementation effective — endothelial dysfunction, ADMA accumulation, reduced eNOS activity — are more likely to be present than at younger ages. However, the same population is more likely to be on medications that interact with arginine, more likely to have underlying cardiovascular conditions that require caution, and less likely to respond to arginine if the ED is neurogenic rather than vasculogenic in origin. The key distinction is severity: mild-to-moderate ED with a vascular component is where the evidence is, not severe ED or ED with a primarily psychological or neurological cause.
How much l-arginine per day is safe?
The NIH indicates that doses up to 9g daily are generally safe for short-to-medium term use. Most clinical trials stay within the 3g to 6g range. Doses above 10g daily increase the likelihood of gastrointestinal side effects and may push hypotensive effects into clinically significant territory in people with blood pressure on the lower end of normal. The sweet spot for most adults using arginine therapeutically — not for acute athletic performance — is 3g to 6g daily in divided doses.
L-arginine and pycnogenol — is the combination worth it?
The combination has specific clinical backing. Multiple studies by Stanislavov and colleagues found that l-arginine combined with Pycnogenol (French maritime pine bark extract) produced significantly greater improvements in erectile function than l-arginine alone. The mechanism is synergistic: pycnogenol enhances eNOS activity and increases the conversion of l-arginine to nitric oxide, meaning the same amount of arginine substrate generates more NO output. At doses of approximately 3g arginine plus 40–120mg pycnogenol daily, the combination has shown effects in men who did not respond to l-arginine alone. For men in the target demographic who want the strongest evidence-based natural approach to vasculogenic ED, this combination is the most clinically substantiated option available without a prescription.
Can l-arginine cause a heart attack?
L-arginine does not cause heart attacks in healthy adults or in the general population. The safety concern is specific and important: in people who have recently had a myocardial infarction, l-arginine supplementation was associated with increased mortality in the VINTAGE MI trial (JAMA, 2006). The proposed mechanism involves arginine’s effects on endothelial function and inflammatory pathways in the acutely injured heart — a context that is mechanistically different from chronic endothelial dysfunction. The contraindication is real and should be respected. For people without recent cardiac events, the cardiovascular evidence for l-arginine is broadly supportive, not harmful.
What foods are naturally highest in l-arginine?
Turkey breast leads among lean protein sources with approximately 2–2.5g per 100g. Pumpkin seeds are the most arginine-dense food per calorie at roughly 2.5g per ounce. Pork loin, chicken breast, salmon, and lean beef all fall in the 1.5–2.5g per 100g range. Plant-based sources include soybeans (approximately 1.7g per half-cup cooked), peanuts (1.4g per ounce), chickpeas, and lentils. Dairy — particularly parmesan and other aged cheeses — contributes meaningfully, as does whole grain rice.
L-arginine vs l-citrulline: which should I take for blood flow?
Citrulline is more bioavailable per gram and raises plasma arginine more effectively than oral arginine does — particularly relevant for exercise performance and general vascular support in healthy adults. L-arginine has more direct clinical evidence in therapeutic doses for specific conditions including vasculogenic ED and hypertension. For men seeking blood flow support in the context of sexual performance, the arginine-pycnogenol combination has the most specific clinical evidence. For healthy adults primarily interested in workout performance, citrulline or citrulline malate is generally the more efficient choice.
L-arginine Benefits: The Bottom Line
L-arginine benefits are real, clinically substantiated, and more precisely targeted than most content suggests. The amino acid works by donating substrate to the eNOS enzyme, which converts it to nitric oxide — a signaling molecule that drives vasodilation, blood pressure reduction, and blood flow to tissues throughout the body, including erectile tissue. The evidence for blood pressure reduction and improvement in vasculogenic erectile dysfunction is the strongest in the l-arginine literature, supported by multiple RCTs and meta-analyses using doses of 3g to 6g daily over 4 to 12 weeks.
The central insight that separates this post from most content on the topic: l-arginine works best when the endothelium is compromised. In healthy adults with normal vascular function, eNOS is already saturated with arginine and adding more does not increase NO production. In adults with hypertension, insulin resistance, vasculogenic ED, or age-related endothelial decline — particularly those over 45 — the arginine-to-ADMA ratio becomes the limiting factor, and supplementation can meaningfully restore NO availability in a system where it has been genuinely depleted.
The post-heart-attack contraindication is real and should not be glossed over. The interaction profile with blood pressure medications, nitrates, and PDE5 inhibitors requires attention. And the dosage gap between typical supplement servings and the doses that actually show clinical effects is a practical consideration that anyone buying arginine supplements should understand.
For adults who fit the profile — vasculogenic ED, prehypertension, endothelial dysfunction, or metabolic syndrome — l-arginine benefits are actionable and backed by legitimate science. For young, healthy athletes looking for performance gains, the case is considerably weaker than the marketing implies, and l-citrulline is a more efficient path to the same mechanism.
Disclaimer: The content on Healthy Routine Lab is for informational and educational purposes only. It is not intended to diagnose, treat, cure, or prevent any medical condition. L-arginine is a dietary supplement, not a medication, and has not been approved by the FDA to treat any disease. Individual results vary. If you have a history of heart disease, are taking blood pressure medications, nitrates, or PDE5 inhibitors, or have any chronic health condition, consult a qualified healthcare provider before starting l-arginine supplementation. People who have recently experienced a myocardial infarction should not take l-arginine without explicit medical guidance.